
From the Open-Publishing Calendar
From the Open-Publishing Newswire
Indybay Feature
Thanks Anna
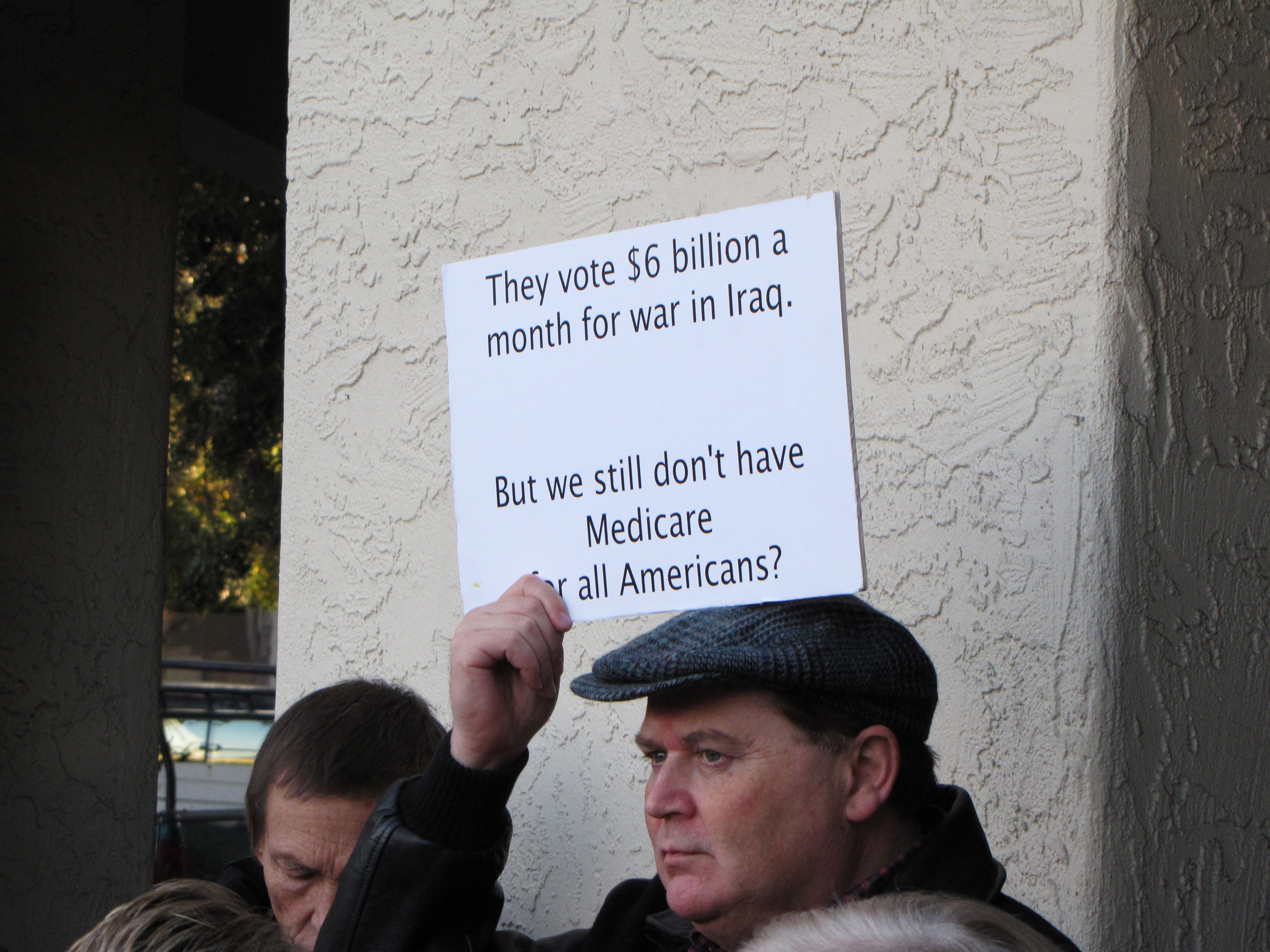
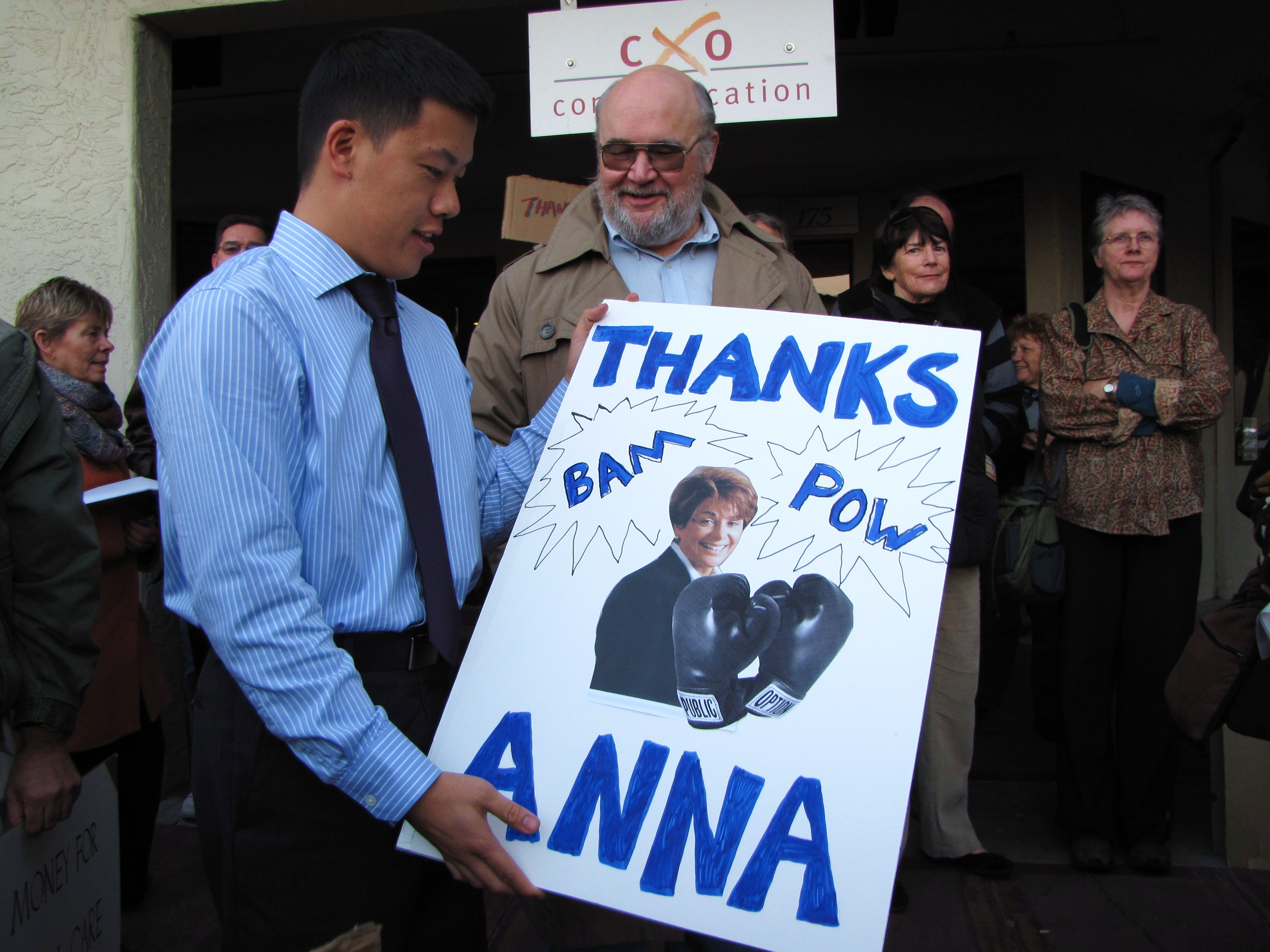
Move On members gathered to thank Anna Eshoo for supporting health care reform.

On Friday, November 13, MoveOn members gathered in front of Anna Eshoo's office to thank her for supporting health care reform. The Raging Grannies of Palo Alto sang songs while the crowd gathered and signed a giant thank you card for Representative Eshoo. It was graciously accepted on her behalf by Anthony Lin, who also had cookies for all the guests! As the sun set, we listened as members shared stories about navigating our broken system, and steeled ourselves to keep pressuring our leaders for better solutions. We know this bill wasn't perfect, and we're committed to continuing this fight until everyone has access to EVERY medically necessary process.
If you want to thank her too, please cut and paste this address into your browser!
http://eshoo.house.gov/index.php?option=com_content&task=view&id=420&Itemid=44
If you want to thank her too, please cut and paste this address into your browser!
http://eshoo.house.gov/index.php?option=com_content&task=view&id=420&Itemid=44




Add Your Comments
Comments
(Hide Comments)
Why I Voted NO on H.R. 3962 (Health Care)
by Congressman Dennis Kucinich
Saturday Nov 14th, 2009 11:36 AM
Outside of the business as usual misinformation coming from medical insurance corporation spokespersons claiming Obama's healthcare plan is "socialist", very few legitimate critiques of Obamacare have made headlines. Here is another "NO" vote against H.R. 3962, though this time for very different reasons.
Kucinich: Why I Voted NO
By November 7, 2009
Straight to the Source
(reposted from Organic Consumer Association)
After voting against H.R. 3962 - Affordable Health Care for America Act, Congressman Dennis Kucinich (D-OH) today made the following statement:
"We have been led to believe that we must make our health care choices only within the current structure of a predatory, for-profit insurance system which makes money not providing health care. We cannot fault the insurance companies for being what they are. But we can fault legislation in which the government incentivizes the perpetuation, indeed the strengthening, of the for-profit health insurance industry, the very source of the problem. When health insurance companies deny care or raise premiums, co-pays and deductibles they are simply trying to make a profit. That is our system.
"Clearly, the insurance companies are the problem, not the solution. They are driving up the cost of health care. Because their massive bureaucracy avoids paying bills so effectively, they force hospitals and doctors to hire their own bureaucracy to fight the insurance companies to avoid getting stuck with an unfair share of the bills. The result is that since 1970, the number of physicians has increased by less than 200% while the number of administrators has increased by 3000%. It is no wonder that 31 cents of every health care dollar goes to administrative costs, not toward providing care. Even those with insurance are at risk. The single biggest cause of bankruptcies in the U.S. is health insurance policies that do not cover you when you get sick.
"But instead of working toward the elimination of for-profit insurance, H.R. 3962 would put the government in the role of accelerating the privatization of health care. In H.R. 3962, the government is requiring at least 21 million Americans to buy private health insurance from the very industry that causes costs to be so high, which will result in at least $70 billion in new annual revenue, much of which is coming from taxpayers. This inevitably will lead to even more costs, more subsidies, and higher profits for insurance companies - a bailout under a blue cross.
"By incurring only a new requirement to cover pre-existing conditions, a weakened public option, and a few other important but limited concessions, the health insurance companies are getting quite a deal. The Center for American Progress' blog, Think Progress, states "since the President signaled that he is backing away from the public option, health insurance stocks have been on the rise." Similarly, healthcare stocks rallied when Senator Max Baucus introduced a bill without a public option. Bloomberg reports that Curtis Lane, a prominent health industry investor, predicted a few weeks ago that "money will start flowing in again" to health insurance stocks after passage of the legislation. Investors.com last month reported that pharmacy benefit managers share prices are hitting all-time highs, with the only industry worry that the Administration would reverse its decision not to negotiate Medicare Part D drug prices, leaving in place a Bush Administration policy.
"During the debate, when the interests of insurance companies would have been effectively challenged, that challenge was turned back. The "robust public option" which would have offered a modicum of competition to a monopolistic industry was whittled down from an initial potential enrollment of 129 million Americans to 6 million. An amendment which would have protected the rights of states to pursue single-payer health care was stripped from the bill at the request of the Administration. Looking ahead, we cringe at the prospect of even greater favors for insurance companies.
"Recent rises in unemployment indicate a widening separation between the finance economy and the real economy. The finance economy considers the health of Wall Street, rising corporate profits, and banks' hoarding of cash, much of it from taxpayers, as sign of an economic recovery. However in the real economy -- in which most Americans live -- the recession is not over. Rising unemployment, business failures, bankruptcies and foreclosures are still hammering Main Street.
"This health care bill continues the redistribution of wealth to Wall Street at the expense of America's manufacturing and service economies which suffer from costs other countries do not have to bear, especially the cost of health care. America continues to stand out among all industrialized nations for its privatized health care system. As a result, we are less competitive in steel, automotive, aerospace and shipping while other countries subsidize their exports in these areas through socializing the cost of health care.
"Notwithstanding the fate of H.R. 3962, America will someday come to recognize the broad social and economic benefits of a not-for-profit, single-payer health care system, which is good for the American people and good for America's businesses, with of course the notable exceptions being insurance and pharmaceuticals."
by Congressman Dennis Kucinich
Saturday Nov 14th, 2009 11:36 AM
Outside of the business as usual misinformation coming from medical insurance corporation spokespersons claiming Obama's healthcare plan is "socialist", very few legitimate critiques of Obamacare have made headlines. Here is another "NO" vote against H.R. 3962, though this time for very different reasons.
Kucinich: Why I Voted NO
By November 7, 2009
Straight to the Source
(reposted from Organic Consumer Association)
After voting against H.R. 3962 - Affordable Health Care for America Act, Congressman Dennis Kucinich (D-OH) today made the following statement:
"We have been led to believe that we must make our health care choices only within the current structure of a predatory, for-profit insurance system which makes money not providing health care. We cannot fault the insurance companies for being what they are. But we can fault legislation in which the government incentivizes the perpetuation, indeed the strengthening, of the for-profit health insurance industry, the very source of the problem. When health insurance companies deny care or raise premiums, co-pays and deductibles they are simply trying to make a profit. That is our system.
"Clearly, the insurance companies are the problem, not the solution. They are driving up the cost of health care. Because their massive bureaucracy avoids paying bills so effectively, they force hospitals and doctors to hire their own bureaucracy to fight the insurance companies to avoid getting stuck with an unfair share of the bills. The result is that since 1970, the number of physicians has increased by less than 200% while the number of administrators has increased by 3000%. It is no wonder that 31 cents of every health care dollar goes to administrative costs, not toward providing care. Even those with insurance are at risk. The single biggest cause of bankruptcies in the U.S. is health insurance policies that do not cover you when you get sick.
"But instead of working toward the elimination of for-profit insurance, H.R. 3962 would put the government in the role of accelerating the privatization of health care. In H.R. 3962, the government is requiring at least 21 million Americans to buy private health insurance from the very industry that causes costs to be so high, which will result in at least $70 billion in new annual revenue, much of which is coming from taxpayers. This inevitably will lead to even more costs, more subsidies, and higher profits for insurance companies - a bailout under a blue cross.
"By incurring only a new requirement to cover pre-existing conditions, a weakened public option, and a few other important but limited concessions, the health insurance companies are getting quite a deal. The Center for American Progress' blog, Think Progress, states "since the President signaled that he is backing away from the public option, health insurance stocks have been on the rise." Similarly, healthcare stocks rallied when Senator Max Baucus introduced a bill without a public option. Bloomberg reports that Curtis Lane, a prominent health industry investor, predicted a few weeks ago that "money will start flowing in again" to health insurance stocks after passage of the legislation. Investors.com last month reported that pharmacy benefit managers share prices are hitting all-time highs, with the only industry worry that the Administration would reverse its decision not to negotiate Medicare Part D drug prices, leaving in place a Bush Administration policy.
"During the debate, when the interests of insurance companies would have been effectively challenged, that challenge was turned back. The "robust public option" which would have offered a modicum of competition to a monopolistic industry was whittled down from an initial potential enrollment of 129 million Americans to 6 million. An amendment which would have protected the rights of states to pursue single-payer health care was stripped from the bill at the request of the Administration. Looking ahead, we cringe at the prospect of even greater favors for insurance companies.
"Recent rises in unemployment indicate a widening separation between the finance economy and the real economy. The finance economy considers the health of Wall Street, rising corporate profits, and banks' hoarding of cash, much of it from taxpayers, as sign of an economic recovery. However in the real economy -- in which most Americans live -- the recession is not over. Rising unemployment, business failures, bankruptcies and foreclosures are still hammering Main Street.
"This health care bill continues the redistribution of wealth to Wall Street at the expense of America's manufacturing and service economies which suffer from costs other countries do not have to bear, especially the cost of health care. America continues to stand out among all industrialized nations for its privatized health care system. As a result, we are less competitive in steel, automotive, aerospace and shipping while other countries subsidize their exports in these areas through socializing the cost of health care.
"Notwithstanding the fate of H.R. 3962, America will someday come to recognize the broad social and economic benefits of a not-for-profit, single-payer health care system, which is good for the American people and good for America's businesses, with of course the notable exceptions being insurance and pharmaceuticals."
i know this bill isn't perfect. i love kucinich and i think his vote here was well-thought out and i respect it.
what i cannot respect is the tone of the left when it makes the perfect the enemy of the good. many of these house members are fearful of standing up for their constituents. we should take every opportunity to remind them that we are paying attention.
you're welcome to join us whenever you want. there is no need to be so insulting and condescending to the people who are willing to be involved.
what i cannot respect is the tone of the left when it makes the perfect the enemy of the good. many of these house members are fearful of standing up for their constituents. we should take every opportunity to remind them that we are paying attention.
you're welcome to join us whenever you want. there is no need to be so insulting and condescending to the people who are willing to be involved.
We are disgusted and mind boggled at the notion that Eshoo should be thanked, and put on a pedastal for signing onto this monstrous and regressive health deform bill. There ought to be non stop protests in front of her office daily, along with all the other corporate shills that signed onto this NO INSURER LEFT BEHIND/NO PHARMA LEFT BEHIND- disguised as health "care" reform. For example, people like Rep. Anna Eshoo and Sen. Kay Hagan, both Democrats along with Pelosi and all the other traitors- – think it’s more important to indefinitely protect the medical-industrial complex from any competition than it is to provide generic versions of life-saving drugs to patients who need them, or to institute real Universal health care that can only happen with a Single Payer- Medicare for All. This legislation would institutionalize the worst aspects of the inhumane, fragmented non-system we have in the US, and cement permanent inequality in access to health care. This horrific plan will further divide the discriminatory non system into tiers all based on one's ability to pay. Premiums, co-pays and out of pocket expenses will continue to sky rocket, and everyone will be required to purchase these inferior, shoddy, over-priced insurance products, or be fined for failing to do so. This legislation makes it illegal to not buy these insurance products. Furthermore, the Big Brother IRS will play a paramount role in everything from certifying incomes for subsidies to monitoring and taxing people who don't purchase insurance. Health insurance is NOT health Care. This legislation doesn't even mention coverage for essential services like vision, hearing and adult dental care except in the most expensive premium plus plans. Imagine the chaos and wasted resources, and bureaucracy that all of this will ensrine, and make it imposssible to undo.MoveOn, and Raging Grannies of PA ought to be fighting tooth and nail to make sure this bogus bill doesn't pass, and that the American people finally get genuine health care reform with a Single Payer, which is the only public option. They ought to be demanding that individual states be permitted to enact Single Payer, nothing Less. And, they ought to be exposing Obamacare for what it is, a corporate bailout. The expression of thanks is totally misplaced since it lends Eshoo and her cronies credibility which is undeserved. It is long overdue to stop this Anybody But Bush mentality, and Anything is better than Nothing for health care reform. In this case, we'd be better off with Nothing than to allow this horrendous bill to move forward. By condoning Eshoo and others you have denigrated all the efforts of the Single Payer advocates who have been banished from the so-called health care debate. The fact is Eshoo has betrayed her constituents, as have almost all of Congress and Obama, with the exception of a few. Enough is Enough! Single Payer- the real option.
Universal Single-Payer Healthcare Coverage: An Economic Stimulus Plan
by Stephen Lendman
Wednesday Nov 18th, 2009 12:26 PM
Imagine - doing the right thing is economically beneficial.
Universal Single Payer Health Care Coverage: An Economic Stimulus Plan - by Stephen Lendman
The Institute for Health & Socio-Economic Policy (IHSP) is "non-profit policy and research group and is the exclusive research arm of the California Nurses Association/National Nurses Organizing Committee, (focusing on) current political/economic policy analysis in health care and other Industries....to enhance, promote and defend the quality of life for all."
In January, it released a "First-of-Its Kind Study" titled, "Single Payer/Medicare for All: An Economic Stimulus Plan for the Nation" to reform the system by providing universal care, adding productive new jobs, billions in public and private revenues, billions more in employee compensation, and added tax revenues. More on that below.
IHSP calls its study an "econometric," not an "arithmetical" health care system analysis, covering both their costs and economic benefits to the nation. Its methodology drew on:
"widely-used and accessible data bases and econometric models which are capable of showing how changes in one economic variable (such as health demand, pricing of services, or taxation of consumers and employers) will affect not only the health care sectors directly, but also their suppliers....their employees and their households, and the generation of federal, state, and local taxes."
Elements of its comprehensive coverage include:
-- universal eligibility; everybody in, no one excluded;
-- everyone under a uniform single standard similar to Medicare Parts A, B, and D; and
-- all enrollees having "the same health services, costs, eligibility requirements, and administrative cost burden.
Indirect Transactions/Activity
These occur when providers buy services or supplies to deliver care:
-- in America, $2.1 trillion in expenditures generates an additional $1.37 trillion in indirect transactions;
-- manufacturing with $307.6 billion benefits most; and
-- in 2006, health care totaled 9.2% of GDP.
Induced Transactions
These are health care worker household consumption transactions, and the indirect sector spending their income:
-- they total an estimated $2.3 trillion; and
-- again, manufacturing benefits most with another $442.8 billion, for an indirect $750.4 billion total.
Total Revenue Generation
IHSP "calculated the economic multiplier to be 2.78, nearly three times the revenues generated within the industry proper." Total direct and indirect health care revenue is $5.856 trillion.
Tax Revenues Generated
-- federal: $538.3 in 2006; and
-- state and local: $826 billion.
Employment
-- 18 million health care workers;
-- another 26 million jobs in other industries for a 45 million total; and
-- nationwide, "health care value added generated 12.1% of employee compensation, and 10.5% of total employment."
Occupations
Health service industries include 511 occupations, 43% in management, administration, finance, physical plant operations, and many other non-health related fields. Registered nurses number about 2.1 million, about 25% of health care professionals. Nursing aides, orderlies, attendants and home health aides comprise another 25%. Doctors are 3% of the total.
Initial Findings
Medicare for all, including Part D will generate:
-- $317 billion in increased public and private revenues;
-- 2.6 million new permanent jobs at an average income of $38,262 annually;
-- $100 billion in worker compensation;
-- $44 billion in new tax revenue - "exclusive of the funding changes to replace employer insurance contributions;"
-- Medicare Part B coverage for 2.6 million Medicare enrollees;
-- Part D coverage for 15 million more;
-- full coverage for the 50 million or more uninsured and millions more underinsured;
-- elimination of the uninsured's uncompensated demands on providers;
-- 27.7 million Medicaid recipients will get the same coverage as others, not the inconsistent kind now offered;
-- elimination of $134.9 billion in state and local expenditures and $175.7 billion for the federal government;
-- for the privately insured, ending problems of eligibility, exclusions, family coverage, premium costs, high out-of-pocket ones, and likelihood to be uninsured if lose employment;
-- for employers, replacing their administrative and financial burden under a shared universal approach;
-- for taxpayers, a reduction of $56 billion in unnecessary, unproductive insurance costs; and
-- for the nation, joining the rest of the industrialized world that provides universal coverage.
Enhanced Medicare for All
-- adding 2.6 million Part A only enrollees and 15 million without Part D will cost about $59 billion, 62% publicly borne;
-- the added expense will generate an additional $154.7 billion in total economic activity, about one million new jobs earning $43.2 billion, and new tax revenues of about $21.2 billion.
Covering the Uninsured
For a net total spending increase (net of the eliminated costs for the uninsured) of $44 billion "in 2006 values," a $120 billion in economic impact will be generated, 945,600 new jobs will be created earning $36.5 billion, and $16.5 billion in taxes will be raised. In addition, the formerly uninsured will pay a small premium above their current expense, but will get greatly enhanced care. Providers will also reduce losses because of non-payments, and emergency rooms will function as intended.
Medicaid
The current system is fragmented, inconsistent, expensive, and fails to provide the full range of preventive and routine care. Discontinuing it at the federal and state levels will generate a "total net direct economic impact" of $16.2 billion dollars breaking down as follows:
-- total new expenditures of $88.9 billion; and
-- discontinuance of $72.7 billion in costs.
Total economic activity will increase by $43 billion. About 336,900 new jobs will be created generating $14.3 billion annually, and tax revenue increases of $6.3 billion.
Medicare Coverage for the Privately Insured
It will bring 196.1 million new enrollees into the new program, standardize their coverage, replace the above enumerated problems, and eliminate an onerous burden on employers that paid (in 2006) 71% of insurance premiums, or $510 billion annually. Burdensome administrative costs will also be eliminated, an estimated $56 billion.
The net effect will shift an employer obligation to public funding and not increase national health costs. It will require more public administrative capacity, and possibly a new or revised tax structure to replace the current privately-financed system.
An Overview of the Health Care Industry
Providers include hospitals, physicians and other health care professionals, nursing care, home health care, ambulatory health services, laboratories and testing facilities, and others. They're closely linked to pharmaceutical, medical equipment, and other producers and suppliers.
Employer-provided coverage is the largest funding source. Privately insured households pay deductibles, or co-pays, and often part of the insurance premium. Taxpayers are the second largest funding source, through federal, state, and local health care programs, including Medicare, Medicaid, and others.
IHSP's report includes a detailed analysis of US health care in 2006, including the composition of the industry, its share of the economy, and the full, direct and indirect, impact that health care activities have on other economic sectors.
Conclusion
IHSP's study concludes that:
"a comprehensive Medicare based Single Payer system can make significant contributions to access of quality care for all US residents and in the process generate a much needed and very substantial economic stimulus in the form of jobs, enhanced business and public revenues and increased wages for the population at large." All this for a small net $63 billion increase yielding much more in benefits.
According to Geri Jenkins, co-president of the National Nurses Organizing Committee/California Nurses Association (NNOC/CNA):
IHSP's analysis shows "for the first time that a single-payer system could not only solve our healthcare crisis, but also substantially contribute to putting America back to work and assisting the economic recovery."
The study's lead author and director of the Institute for Health and Socio-Economic Policy (the NNOC/CNA research arm), Don DeMoro, added:
"If we were to expand our present Medicare system to cover all Americans, the economic stimulus alone would create an immense engine that would help drive our national economy for decades to come."
All for a tiny fraction of the Wall Street bailouts that looted the federal Treasury, gravely harmed the country, and delayed for a future time a far more serious day of reckoning.
Physicians for a National Health Program (PNHP) Support for Universal Single-Payer Coverage
PNHP calls the current system "outrageously expensive, yet inadequate" because of the 50 million or more uninsured and another 30 million or more underinsured. It spends more and delivers less through:
"a patchwork system of for-profit payers. Private insurers necessarily waste health dollars on things (unrelated to care): overhead, underwriting, billing, sales and marketing (plus) huge profits and exorbitant executive pay. Doctors and hospitals must maintain costly administrative staffs to deal with the bureaucracy (consuming nearly one-third) of Americans' health dollars." The potential savings from single-payer financing is "more than $350 billion per year....enough to" cover everyone at no more than the current cost and perhaps less depending on services provided and if government negotiates lower drug prices the way other countries do.
Consider the benefits - single-payer will cover "all medically necessary services, including: doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs. Patients" will have free choice of providers, and doctors will "regain autonomy over patient care," no longer restricted by insurance company gatekeepers. Overall, health care in America will achieve a quantum leap improvement compared to the dysfuntional state it's now in, worse still if Obamacare passes.
"HR 3962: Affordable Health Care for America Act" - The Public Betrayal Act to Enrich the Insurance, Drug, and Large Hospital Chain Cartels
On November 7, by a narrow 51 - 49% majority, the House passed legislation former CIGNA executive, now critic, Wendall Potter calls "the Insurance Company Profit Protection and Enhancement Act." Add the drug and hospital chain cartels that will profit hugely if it's enacted.
Voting for it - 219 Democrats and one Republican. Against it were the remaining Republicans and 39 Democrats.
Among its supporters were cosponsors of "HR 676: United States National Health Care Act or the Expanded and Improved Medicare for All Act," including universal single-payer advocates:
-- Anthony Weiner (D. NY);
-- Danny Davis (D. IL), this writer's representative;
-- Jesse Jackson, Jr. (D. IL);
-- Barney Frank (D. MA); and
-- Barbara Lee (D. CA).
Dennis Kucinich (D. OH) explained "Why I Voted No," saying:
The current "for-profit insurance system....makes money (by denying) health care." HR 3962 strengthens the source of the problem. "Clearly, the insurance companies are the problem, not the solution. They are driving up the cost of health care." They're the reason why "31 cents of every health care dollar goes to administrative costs, not toward providing care. Even those with insurance are at risk. The single biggest cause of bankruptcies in the US is health policies that do not cover you when you get sick."
Instead of fixing the problem, HR 3962 "accelerate(s) the privatization of health care. (It) inevitably will lead to even more costs, more subsidies, and higher profits for insurance companies - a bailout under a blue cross. (The bill) continues the redistribution of wealth to Wall Street at the expense of" Americans getting the kind of health care they deserve and badly need.
Former president of Physicians for a National Health Program, Dr. John Geyman, cited HR 3962 saying "No Bill is Better Than a Bad Bill" in enumerating its negatives, including:
-- enriching providers "on the backs of patients and their families;"
-- having "no effective cost containment mechanisms;"
-- a public option available only to about six million people or 2% of the population, and in 2013 will cost more than private programs for sicker people because insurers are unrestricted on what they can charge;
-- health care will be more, not less expensive; and
-- will still leave millions uninsured and millions more underinsured.
"In sum, this (monster won't) fix the major problems of cost and affordable access. (It) will add new layers of bureaucracy and complexity, is not fiscally responsible, and is not sustainable."
Debate now shifts to the Senate where the best outcome will be killing Obamacare because "no bill is better than a bad" one.
The California Nurses Association (NSA) said the following:
"This Bill Fails to Control Costs." While providing "limited assistance for some, the inconvenient truth is (it falls) far short in effective controls on skyrocketing insurance, pharmaceutical and hospital costs, (does) little to stop insurance companies from denying needed medical care recommended by doctors, and (provides) little relief for Americans with employer-sponsored insurance worried about health security for themselves and their families." And the Senate legislation is even worse.
The National Organization for Women said the "Bill Obliterates Women's Fundamental Right to Choose" that became law in the landmark 1973 Roe v. Wade decision, and is still the law of the land. The Court held that a woman may abort her pregnancy for any reason, up to when "the fetus becomes viable."
HR 3962 violates that right. Except in cases of rape, incest, or if a woman faces death, the Stupak (D. MI) amendment prohibits using federal money for insurance covering abortion. It prevents women participating in insurance exchanges from using their own money to buy abortion coverage. It denies low-income women access to it entirely.
According to the Congressional Budget Office (CBO), it:
-- will cost $1.055 trillion over the next decade, netting out at $894 billion after revenue enhancements;
-- mandates coverage and penalizes those without it up to 2.5% of their income;
-- insurance for individuals earning $44,000 pre-tax will be $5,300, plus another $2,000 in out-of-pocket expenses for an annual $7,300 total, or 17% of their annual income; families earning $102,000 pre-tax will pay $15,000 in premiums plus another $5,300 in out-of-pocket costs for a total annual $20,300 cost, or 20% of their annual income; those earning below these amounts will be eligible for subsidies, based on a sliding scale, paid directly to insurers;
-- includes a watered-down public option by setting up insurance exchanges through which low income households are subsidized to make coverage more affordable; the plan is so weak, only an estimated 6 million or fewer will qualify; Physicians for a National Health Program (PNHP) lists myths and facts about it below;
-- expands eligibility for Medicaid;
-- lowers the federal deficit by $104 billion by 2019 and even more in the following ten years;
-- "substantially reduce(s) the growth of Medicare's payment rates for most services" by cutting over $400 billion in costs; the true figure is much higher; more on that below; and
-- leaves 18 million uninsured by 2019, including about six million undocumented immigrants; the Senate Finance Committee's bill leaves 25 million uninsured.
Pre-existing condition exclusions will be prohibited, but insurers may charge what they wish, so effectively nothing changes. Endorsing the bill:
-- the drug cartel;
-- the American Medical Association;
-- the US Conference of Catholic Bishops because of the anti-abortion provision; and
-- the AARP, an insurance/financial broker masquerading as an advocacy group for anyone aged 50 or older.
The Centers for Medicare & Medicaid Services' (CMS) Assessment of Medicare Cuts Under HR 3962
On November 13, CMS released estimates of the "costs, savings, and coverage impacts" of HR 3962, showing Medicare spending will be cut by a draconian $570.6 billion, well above the CBO figure. Enrollees unable to cover the difference will be devastated. Millions will get less care when they most need it. In some cases, hospitals and nursing homes may deny it altogether.
Medicare will introduce "permanent annual productivity adjustments to price updates for institutional providers" to maximize "efficiency" - costing $282 billion, over half the total cuts. They'll affect acute care hospitals, nursing facilities, and home health agencies, and be based on economic productivity overall, but CMS notes that:
"Except in the case of physician services, we are not aware of any empirical evidence demonstrating the medical community's ability to achieve productivity improvements equal to those of (the) overall economy."
As a result, provider costs will rise faster than Medicare payment increases. They, in turn, will reduce care or opt out of the program altogether. Many providers have done it because of low compensation. CMS states:
"Providers for whom Medicare constitutes a substantive portion of their business could find it difficult to remain profitable and might end their participation in the program (possibly jeopardizing access to care for beneficiaries)."
Medicaid eligibility will also be impacted, threatening access for millions of poor people, dependent on it as their sole source of care. Although HR 3962 increases spending by $77.5 billion to cover the cost of new enrollees, CMS says higher demand may cause providers:
"to accept more patients who have private insurance (with relatively attractive payment rates) and fewer Medicaid" ones because it won't be cost effective to do it.
Physicians for a National Health Program (PNHP) on Myths and Facts about a Public Option
Myth: More choice.
Fact check:
Provider and location choices will be limited. Seeking care outside networks will cost more, and authorization will still be required.
Myth: Patients may keep their doctors regardless of employment changes or health.
Fact check:
The employer-based system stays intact. If a new plan is chosen, only doctors in it may be accessed. Patients retaining their own will incur higher out-of-network fees. Insurers may also cherry pick the healthy and avoid the sick. Patients becoming ill risk losing employer-based coverage or face higher premiums to keep it.
Myth: Private insurers will have to compete on a level playing field.
Fact check:
HMO's "undermine fair competition despite regulations." They "cherry-pick" the healthy and avoid the high-risk. They also cost up to 19% more than traditional Medicare despite their lower age category enrollees.
Myth: Everyone will have quality, affordable care.
Fact check:
The current system is unsustainable. It will worsen if Obamacare passes. In whatever form, the "international experience with public option schemes" shows they don't provide universal coverage - because insurers pick the best and screen out the rest.
Myth: Patients will get better care because of "innovation in the quality care physicians provide."
Fact check:
Quality won't improve. Today's dysfunctional system won't change. It's driven by profits, high costs, and for insurers denying expensive care or delaying it as long as possible.
Myth: Cost will be reduced.
Fact Check:
False because no provider bureaucracy savings will be achieved. "Adding a public option to the array of private insurance companies....will only exacerbate the waste and inefficiency inherent in a patchwork system...."
Final Comments
Health care is a fundamental human right no different than food, shelter, clothing, clean air and water, and other essentials to life and well-being, not something to be bought and sold as a commodity. Universal single-payer coverage is the solution, not America's dysfunctional for-profit model.
If Obamacare is enacted, it will cost more, deliver less, leave millions uninsured, millions more underinsured and leave a broken system in place. It will enrich the insurance, drug and large hospital chain cartels at the expense of universal coverage. It will solidify a class-based system delivering the best care money can buy. Others will get sub-standard treatment, and for millions none at all. The solution is everybody in, nobody out under a universal, single-payer system. No one should accept less or politicians who won't provide it.
Stephen Lendman is a Research Associate of the Centre for Research on Globalization. He lives in Chicago and can be reached at lendmanstephen [at] sbcglobal.net.
Also visit his blog site at sjlendman.blogspot.com and listen to The Global Research News Hour on RepublicBroadcasting.org Monday - Friday at 10AM US Central time for cutting-edge discussions with distinguished guests on world and national issues. All programs are archived for easy listening.
http://republicbroadcasting.org/Global%20Research/index.php?cmd=archives.year&ProgramID=33&year=9
http://sjlendman.blogspot.com
by Stephen Lendman
Wednesday Nov 18th, 2009 12:26 PM
Imagine - doing the right thing is economically beneficial.
Universal Single Payer Health Care Coverage: An Economic Stimulus Plan - by Stephen Lendman
The Institute for Health & Socio-Economic Policy (IHSP) is "non-profit policy and research group and is the exclusive research arm of the California Nurses Association/National Nurses Organizing Committee, (focusing on) current political/economic policy analysis in health care and other Industries....to enhance, promote and defend the quality of life for all."
In January, it released a "First-of-Its Kind Study" titled, "Single Payer/Medicare for All: An Economic Stimulus Plan for the Nation" to reform the system by providing universal care, adding productive new jobs, billions in public and private revenues, billions more in employee compensation, and added tax revenues. More on that below.
IHSP calls its study an "econometric," not an "arithmetical" health care system analysis, covering both their costs and economic benefits to the nation. Its methodology drew on:
"widely-used and accessible data bases and econometric models which are capable of showing how changes in one economic variable (such as health demand, pricing of services, or taxation of consumers and employers) will affect not only the health care sectors directly, but also their suppliers....their employees and their households, and the generation of federal, state, and local taxes."
Elements of its comprehensive coverage include:
-- universal eligibility; everybody in, no one excluded;
-- everyone under a uniform single standard similar to Medicare Parts A, B, and D; and
-- all enrollees having "the same health services, costs, eligibility requirements, and administrative cost burden.
Indirect Transactions/Activity
These occur when providers buy services or supplies to deliver care:
-- in America, $2.1 trillion in expenditures generates an additional $1.37 trillion in indirect transactions;
-- manufacturing with $307.6 billion benefits most; and
-- in 2006, health care totaled 9.2% of GDP.
Induced Transactions
These are health care worker household consumption transactions, and the indirect sector spending their income:
-- they total an estimated $2.3 trillion; and
-- again, manufacturing benefits most with another $442.8 billion, for an indirect $750.4 billion total.
Total Revenue Generation
IHSP "calculated the economic multiplier to be 2.78, nearly three times the revenues generated within the industry proper." Total direct and indirect health care revenue is $5.856 trillion.
Tax Revenues Generated
-- federal: $538.3 in 2006; and
-- state and local: $826 billion.
Employment
-- 18 million health care workers;
-- another 26 million jobs in other industries for a 45 million total; and
-- nationwide, "health care value added generated 12.1% of employee compensation, and 10.5% of total employment."
Occupations
Health service industries include 511 occupations, 43% in management, administration, finance, physical plant operations, and many other non-health related fields. Registered nurses number about 2.1 million, about 25% of health care professionals. Nursing aides, orderlies, attendants and home health aides comprise another 25%. Doctors are 3% of the total.
Initial Findings
Medicare for all, including Part D will generate:
-- $317 billion in increased public and private revenues;
-- 2.6 million new permanent jobs at an average income of $38,262 annually;
-- $100 billion in worker compensation;
-- $44 billion in new tax revenue - "exclusive of the funding changes to replace employer insurance contributions;"
-- Medicare Part B coverage for 2.6 million Medicare enrollees;
-- Part D coverage for 15 million more;
-- full coverage for the 50 million or more uninsured and millions more underinsured;
-- elimination of the uninsured's uncompensated demands on providers;
-- 27.7 million Medicaid recipients will get the same coverage as others, not the inconsistent kind now offered;
-- elimination of $134.9 billion in state and local expenditures and $175.7 billion for the federal government;
-- for the privately insured, ending problems of eligibility, exclusions, family coverage, premium costs, high out-of-pocket ones, and likelihood to be uninsured if lose employment;
-- for employers, replacing their administrative and financial burden under a shared universal approach;
-- for taxpayers, a reduction of $56 billion in unnecessary, unproductive insurance costs; and
-- for the nation, joining the rest of the industrialized world that provides universal coverage.
Enhanced Medicare for All
-- adding 2.6 million Part A only enrollees and 15 million without Part D will cost about $59 billion, 62% publicly borne;
-- the added expense will generate an additional $154.7 billion in total economic activity, about one million new jobs earning $43.2 billion, and new tax revenues of about $21.2 billion.
Covering the Uninsured
For a net total spending increase (net of the eliminated costs for the uninsured) of $44 billion "in 2006 values," a $120 billion in economic impact will be generated, 945,600 new jobs will be created earning $36.5 billion, and $16.5 billion in taxes will be raised. In addition, the formerly uninsured will pay a small premium above their current expense, but will get greatly enhanced care. Providers will also reduce losses because of non-payments, and emergency rooms will function as intended.
Medicaid
The current system is fragmented, inconsistent, expensive, and fails to provide the full range of preventive and routine care. Discontinuing it at the federal and state levels will generate a "total net direct economic impact" of $16.2 billion dollars breaking down as follows:
-- total new expenditures of $88.9 billion; and
-- discontinuance of $72.7 billion in costs.
Total economic activity will increase by $43 billion. About 336,900 new jobs will be created generating $14.3 billion annually, and tax revenue increases of $6.3 billion.
Medicare Coverage for the Privately Insured
It will bring 196.1 million new enrollees into the new program, standardize their coverage, replace the above enumerated problems, and eliminate an onerous burden on employers that paid (in 2006) 71% of insurance premiums, or $510 billion annually. Burdensome administrative costs will also be eliminated, an estimated $56 billion.
The net effect will shift an employer obligation to public funding and not increase national health costs. It will require more public administrative capacity, and possibly a new or revised tax structure to replace the current privately-financed system.
An Overview of the Health Care Industry
Providers include hospitals, physicians and other health care professionals, nursing care, home health care, ambulatory health services, laboratories and testing facilities, and others. They're closely linked to pharmaceutical, medical equipment, and other producers and suppliers.
Employer-provided coverage is the largest funding source. Privately insured households pay deductibles, or co-pays, and often part of the insurance premium. Taxpayers are the second largest funding source, through federal, state, and local health care programs, including Medicare, Medicaid, and others.
IHSP's report includes a detailed analysis of US health care in 2006, including the composition of the industry, its share of the economy, and the full, direct and indirect, impact that health care activities have on other economic sectors.
Conclusion
IHSP's study concludes that:
"a comprehensive Medicare based Single Payer system can make significant contributions to access of quality care for all US residents and in the process generate a much needed and very substantial economic stimulus in the form of jobs, enhanced business and public revenues and increased wages for the population at large." All this for a small net $63 billion increase yielding much more in benefits.
According to Geri Jenkins, co-president of the National Nurses Organizing Committee/California Nurses Association (NNOC/CNA):
IHSP's analysis shows "for the first time that a single-payer system could not only solve our healthcare crisis, but also substantially contribute to putting America back to work and assisting the economic recovery."
The study's lead author and director of the Institute for Health and Socio-Economic Policy (the NNOC/CNA research arm), Don DeMoro, added:
"If we were to expand our present Medicare system to cover all Americans, the economic stimulus alone would create an immense engine that would help drive our national economy for decades to come."
All for a tiny fraction of the Wall Street bailouts that looted the federal Treasury, gravely harmed the country, and delayed for a future time a far more serious day of reckoning.
Physicians for a National Health Program (PNHP) Support for Universal Single-Payer Coverage
PNHP calls the current system "outrageously expensive, yet inadequate" because of the 50 million or more uninsured and another 30 million or more underinsured. It spends more and delivers less through:
"a patchwork system of for-profit payers. Private insurers necessarily waste health dollars on things (unrelated to care): overhead, underwriting, billing, sales and marketing (plus) huge profits and exorbitant executive pay. Doctors and hospitals must maintain costly administrative staffs to deal with the bureaucracy (consuming nearly one-third) of Americans' health dollars." The potential savings from single-payer financing is "more than $350 billion per year....enough to" cover everyone at no more than the current cost and perhaps less depending on services provided and if government negotiates lower drug prices the way other countries do.
Consider the benefits - single-payer will cover "all medically necessary services, including: doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs. Patients" will have free choice of providers, and doctors will "regain autonomy over patient care," no longer restricted by insurance company gatekeepers. Overall, health care in America will achieve a quantum leap improvement compared to the dysfuntional state it's now in, worse still if Obamacare passes.
"HR 3962: Affordable Health Care for America Act" - The Public Betrayal Act to Enrich the Insurance, Drug, and Large Hospital Chain Cartels
On November 7, by a narrow 51 - 49% majority, the House passed legislation former CIGNA executive, now critic, Wendall Potter calls "the Insurance Company Profit Protection and Enhancement Act." Add the drug and hospital chain cartels that will profit hugely if it's enacted.
Voting for it - 219 Democrats and one Republican. Against it were the remaining Republicans and 39 Democrats.
Among its supporters were cosponsors of "HR 676: United States National Health Care Act or the Expanded and Improved Medicare for All Act," including universal single-payer advocates:
-- Anthony Weiner (D. NY);
-- Danny Davis (D. IL), this writer's representative;
-- Jesse Jackson, Jr. (D. IL);
-- Barney Frank (D. MA); and
-- Barbara Lee (D. CA).
Dennis Kucinich (D. OH) explained "Why I Voted No," saying:
The current "for-profit insurance system....makes money (by denying) health care." HR 3962 strengthens the source of the problem. "Clearly, the insurance companies are the problem, not the solution. They are driving up the cost of health care." They're the reason why "31 cents of every health care dollar goes to administrative costs, not toward providing care. Even those with insurance are at risk. The single biggest cause of bankruptcies in the US is health policies that do not cover you when you get sick."
Instead of fixing the problem, HR 3962 "accelerate(s) the privatization of health care. (It) inevitably will lead to even more costs, more subsidies, and higher profits for insurance companies - a bailout under a blue cross. (The bill) continues the redistribution of wealth to Wall Street at the expense of" Americans getting the kind of health care they deserve and badly need.
Former president of Physicians for a National Health Program, Dr. John Geyman, cited HR 3962 saying "No Bill is Better Than a Bad Bill" in enumerating its negatives, including:
-- enriching providers "on the backs of patients and their families;"
-- having "no effective cost containment mechanisms;"
-- a public option available only to about six million people or 2% of the population, and in 2013 will cost more than private programs for sicker people because insurers are unrestricted on what they can charge;
-- health care will be more, not less expensive; and
-- will still leave millions uninsured and millions more underinsured.
"In sum, this (monster won't) fix the major problems of cost and affordable access. (It) will add new layers of bureaucracy and complexity, is not fiscally responsible, and is not sustainable."
Debate now shifts to the Senate where the best outcome will be killing Obamacare because "no bill is better than a bad" one.
The California Nurses Association (NSA) said the following:
"This Bill Fails to Control Costs." While providing "limited assistance for some, the inconvenient truth is (it falls) far short in effective controls on skyrocketing insurance, pharmaceutical and hospital costs, (does) little to stop insurance companies from denying needed medical care recommended by doctors, and (provides) little relief for Americans with employer-sponsored insurance worried about health security for themselves and their families." And the Senate legislation is even worse.
The National Organization for Women said the "Bill Obliterates Women's Fundamental Right to Choose" that became law in the landmark 1973 Roe v. Wade decision, and is still the law of the land. The Court held that a woman may abort her pregnancy for any reason, up to when "the fetus becomes viable."
HR 3962 violates that right. Except in cases of rape, incest, or if a woman faces death, the Stupak (D. MI) amendment prohibits using federal money for insurance covering abortion. It prevents women participating in insurance exchanges from using their own money to buy abortion coverage. It denies low-income women access to it entirely.
According to the Congressional Budget Office (CBO), it:
-- will cost $1.055 trillion over the next decade, netting out at $894 billion after revenue enhancements;
-- mandates coverage and penalizes those without it up to 2.5% of their income;
-- insurance for individuals earning $44,000 pre-tax will be $5,300, plus another $2,000 in out-of-pocket expenses for an annual $7,300 total, or 17% of their annual income; families earning $102,000 pre-tax will pay $15,000 in premiums plus another $5,300 in out-of-pocket costs for a total annual $20,300 cost, or 20% of their annual income; those earning below these amounts will be eligible for subsidies, based on a sliding scale, paid directly to insurers;
-- includes a watered-down public option by setting up insurance exchanges through which low income households are subsidized to make coverage more affordable; the plan is so weak, only an estimated 6 million or fewer will qualify; Physicians for a National Health Program (PNHP) lists myths and facts about it below;
-- expands eligibility for Medicaid;
-- lowers the federal deficit by $104 billion by 2019 and even more in the following ten years;
-- "substantially reduce(s) the growth of Medicare's payment rates for most services" by cutting over $400 billion in costs; the true figure is much higher; more on that below; and
-- leaves 18 million uninsured by 2019, including about six million undocumented immigrants; the Senate Finance Committee's bill leaves 25 million uninsured.
Pre-existing condition exclusions will be prohibited, but insurers may charge what they wish, so effectively nothing changes. Endorsing the bill:
-- the drug cartel;
-- the American Medical Association;
-- the US Conference of Catholic Bishops because of the anti-abortion provision; and
-- the AARP, an insurance/financial broker masquerading as an advocacy group for anyone aged 50 or older.
The Centers for Medicare & Medicaid Services' (CMS) Assessment of Medicare Cuts Under HR 3962
On November 13, CMS released estimates of the "costs, savings, and coverage impacts" of HR 3962, showing Medicare spending will be cut by a draconian $570.6 billion, well above the CBO figure. Enrollees unable to cover the difference will be devastated. Millions will get less care when they most need it. In some cases, hospitals and nursing homes may deny it altogether.
Medicare will introduce "permanent annual productivity adjustments to price updates for institutional providers" to maximize "efficiency" - costing $282 billion, over half the total cuts. They'll affect acute care hospitals, nursing facilities, and home health agencies, and be based on economic productivity overall, but CMS notes that:
"Except in the case of physician services, we are not aware of any empirical evidence demonstrating the medical community's ability to achieve productivity improvements equal to those of (the) overall economy."
As a result, provider costs will rise faster than Medicare payment increases. They, in turn, will reduce care or opt out of the program altogether. Many providers have done it because of low compensation. CMS states:
"Providers for whom Medicare constitutes a substantive portion of their business could find it difficult to remain profitable and might end their participation in the program (possibly jeopardizing access to care for beneficiaries)."
Medicaid eligibility will also be impacted, threatening access for millions of poor people, dependent on it as their sole source of care. Although HR 3962 increases spending by $77.5 billion to cover the cost of new enrollees, CMS says higher demand may cause providers:
"to accept more patients who have private insurance (with relatively attractive payment rates) and fewer Medicaid" ones because it won't be cost effective to do it.
Physicians for a National Health Program (PNHP) on Myths and Facts about a Public Option
Myth: More choice.
Fact check:
Provider and location choices will be limited. Seeking care outside networks will cost more, and authorization will still be required.
Myth: Patients may keep their doctors regardless of employment changes or health.
Fact check:
The employer-based system stays intact. If a new plan is chosen, only doctors in it may be accessed. Patients retaining their own will incur higher out-of-network fees. Insurers may also cherry pick the healthy and avoid the sick. Patients becoming ill risk losing employer-based coverage or face higher premiums to keep it.
Myth: Private insurers will have to compete on a level playing field.
Fact check:
HMO's "undermine fair competition despite regulations." They "cherry-pick" the healthy and avoid the high-risk. They also cost up to 19% more than traditional Medicare despite their lower age category enrollees.
Myth: Everyone will have quality, affordable care.
Fact check:
The current system is unsustainable. It will worsen if Obamacare passes. In whatever form, the "international experience with public option schemes" shows they don't provide universal coverage - because insurers pick the best and screen out the rest.
Myth: Patients will get better care because of "innovation in the quality care physicians provide."
Fact check:
Quality won't improve. Today's dysfunctional system won't change. It's driven by profits, high costs, and for insurers denying expensive care or delaying it as long as possible.
Myth: Cost will be reduced.
Fact Check:
False because no provider bureaucracy savings will be achieved. "Adding a public option to the array of private insurance companies....will only exacerbate the waste and inefficiency inherent in a patchwork system...."
Final Comments
Health care is a fundamental human right no different than food, shelter, clothing, clean air and water, and other essentials to life and well-being, not something to be bought and sold as a commodity. Universal single-payer coverage is the solution, not America's dysfunctional for-profit model.
If Obamacare is enacted, it will cost more, deliver less, leave millions uninsured, millions more underinsured and leave a broken system in place. It will enrich the insurance, drug and large hospital chain cartels at the expense of universal coverage. It will solidify a class-based system delivering the best care money can buy. Others will get sub-standard treatment, and for millions none at all. The solution is everybody in, nobody out under a universal, single-payer system. No one should accept less or politicians who won't provide it.
Stephen Lendman is a Research Associate of the Centre for Research on Globalization. He lives in Chicago and can be reached at lendmanstephen [at] sbcglobal.net.
Also visit his blog site at sjlendman.blogspot.com and listen to The Global Research News Hour on RepublicBroadcasting.org Monday - Friday at 10AM US Central time for cutting-edge discussions with distinguished guests on world and national issues. All programs are archived for easy listening.
http://republicbroadcasting.org/Global%20Research/index.php?cmd=archives.year&ProgramID=33&year=9
http://sjlendman.blogspot.com
We are 100% volunteer and depend on your participation to sustain our efforts!
Donate

$125.00 donated
in the past month
Get Involved
If you'd like to help with maintaining or developing the website, contact us.
Publish
Publish your stories and upcoming events on Indybay.
Topics
More
Search Indybay's Archives
Advanced Search
►
▼
IMC Network